Why a Prescription Isn't an Answer
This is not an argument against medication.
Medication has its place in men's sexual health. For some men, in the right clinical context with a clear understanding of what's driving their symptoms, it is a legitimate and useful tool. Nothing in this article is intended to dismiss that.
This is about what happens when a prescription becomes the entire clinical response to a question that nobody actually investigated. When the system hands a man a solution before anyone has identified the problem.
That happens more often than it should. And it has consequences worth understanding.
What Usually Happens in the Current System
A man finally decides to bring up sexual health concerns with his doctor. This takes more courage than it should, but he does it. He describes what he has been experiencing. The drive has changed. Things aren't working the way they used to. Something feels different.
The doctor, working within a system that allocates 15 minutes to this conversation and offers few tools beyond the prescription pad, does what the system makes easiest. A prescription is written. Maybe a brief explanation of how the medication works. A follow-up scheduled that may or may not happen.
No bloodwork. No investigation into hormone levels, vascular health, thyroid function, or metabolic status. No clinical picture of what is actually generating the symptoms. A prescription, and an implicit message that this is the appropriate response to what the man described.
The man leaves with something. Whether it addresses anything real, whether there is something more significant underneath the symptom, whether the underlying cause is progressing while the surface symptom is being managed, those questions go unasked.
This is not an indictment of primary care physicians. They are operating within genuine structural constraints. It is an observation about a system that has settled on a pill as an adequate response to a signal the body is sending for a reason.
The Fundamental Problem
Dr. Lee-Agawa is direct on this point, and it is worth stating plainly: a prescription for sexual dysfunction without a clinical workup is not a diagnosis. It is a best guess with a co-pay attached.
Sexual dissatisfaction and erectile dysfunction are not conditions that exist in isolation from the rest of the body. They are outputs. They reflect the cumulative state of the hormonal, vascular, metabolic, and thyroid systems that govern how a man's physiology functions day to day. When those systems are not performing correctly, sexual health is frequently one of the first areas where the disruption becomes visible.
This is actually important clinical information, if anyone is reading it as such.
Treating the visible symptom without examining what is generating it means the underlying issue continues operating unchecked. The vascular dysfunction that is quietly progressing. The hormonal imbalance that has been building across years. The metabolic disruption that is affecting multiple systems simultaneously. None of that pauses because the symptom is being managed.
A prescription does not address any of it. It produces a temporary effect through a specific chemical pathway while the actual clinical picture remains entirely unexamined.
What the Medication Actually Does and Doesn't Do
Understanding the mechanism of the most commonly prescribed medications makes the limitation clear.
PDE5 inhibitors, the class that includes the most widely recognized erectile dysfunction medications, work by blocking an enzyme that restricts blood flow to specific tissue. In the presence of arousal, this blocking effect allows increased blood flow to produce the intended result.
This is a real mechanism with real effects. For men whose primary issue is a specific and isolated vascular limitation and whose overall physiology is otherwise functioning well, it can produce meaningful results.
What it does not do is equally important to understand.
It does not address testosterone levels, free or total. It does not address SHBG, which determines how much of the available testosterone the body can actually use. It does not address estradiol balance, which affects drive, mood, and body composition in men more significantly than most people realize. It does not address pituitary signaling through FSH and LH. It does not affect thyroid function, insulin resistance, metabolic health, or cardiovascular status.
It produces an effect through one pathway while everything upstream of that pathway remains exactly as it was before the prescription was written.
For a man whose primary driver is low free testosterone, the medication is working around a hormonal problem that has a direct clinical solution. For a man whose primary driver is metabolic dysfunction affecting vascular health, the medication is producing a temporary effect while the underlying vascular picture continues developing. For a man with thyroid dysfunction mimicking the symptoms of hormonal decline, the medication is addressing the wrong system entirely.
Knowing which situation you are actually in requires a clinical picture. And a clinical picture requires someone to look for one.
The Cost of Managing Without Understanding
There is a compounding cost to treating the symptom while the cause remains unaddressed, and it is worth being explicit about what that cost looks like over time.
The conditions that most commonly drive sexual dissatisfaction in men, hormonal decline, vascular dysfunction, metabolic dysregulation, insulin resistance, thyroid imbalance, do not stay static while the symptom is being managed. They develop. The hormonal baseline that is addressable today may be more entrenched in two years. The vascular health that is recoverable now is more difficult to reverse later. The metabolic factors that are currently mild become more significant as they compound.
Time matters in ways that are not immediately visible in the short term but become clinically significant over years. Men who get a complete clinical picture early and address what they find have more to work with. The window for meaningful intervention is wider. The outcomes available to them are better.
A prescription bought time. It did not buy health. And for many men, it quietly closed a window they did not know was open.
What a Real Clinical Response Looks Like
At Springhouse the starting point is consistent: understand the patient before recommending anything.
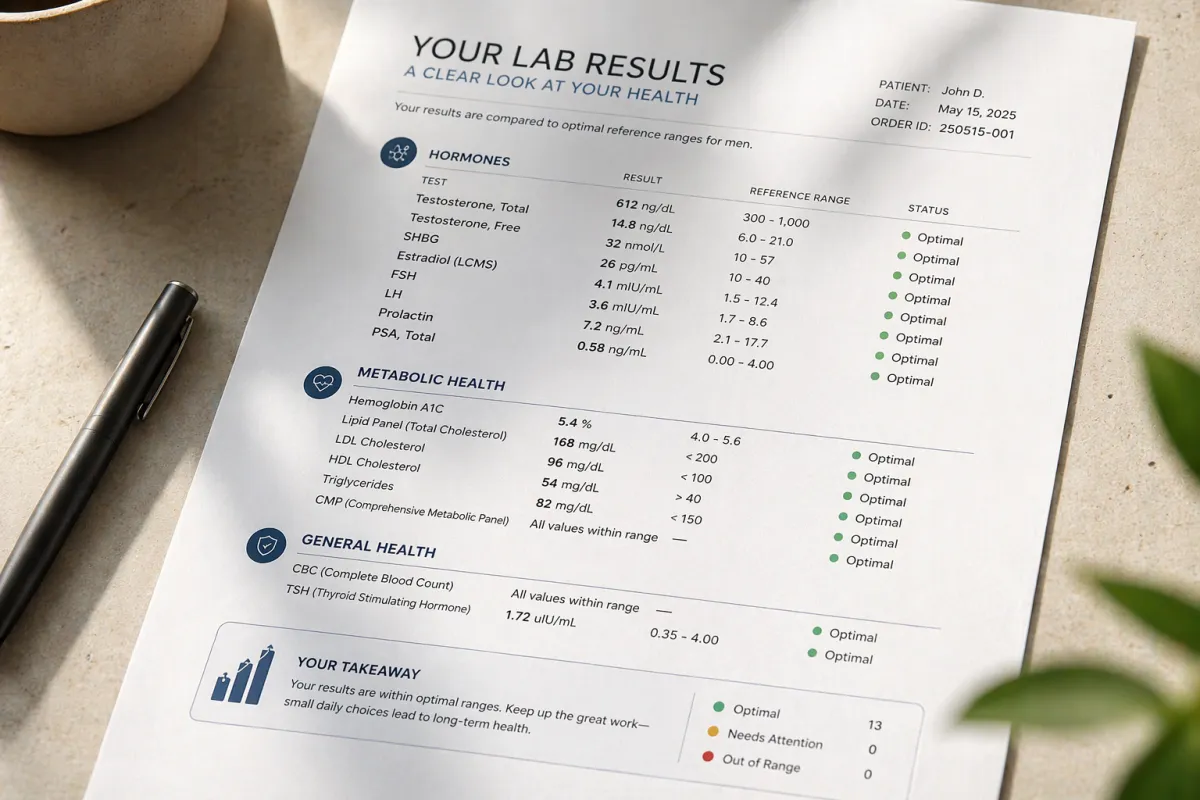
We strongly recommend comprehensive bloodwork as part of every consultation before any treatment decision is made. Testosterone free and total with Sex Hormone Binding Globulin (SHBG). Estradiol. Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH). Prolactin. Prostate Specific Antigen (PSA). A full Complete Blood Count (CBC), Comprehensive Metabolic Panel (CMP), lipid panel, Thyroid Stimulating Hormone (TSH), and Hemoglobin A1C.
This panel gives a complete picture of the hormonal, metabolic, cardiovascular, and thyroid factors that drive how a man feels, functions, and performs. It tells us what is actually happening, not what we might assume based on the symptom presented.
From that picture the treatment plan is built around the individual patient.
For some men the primary clinical intervention is RF treatment using the Apex by InMode platform, which addresses the vascular and tissue factors that contribute to sexual dysfunction non-invasively, without surgery, without recovery, and without the limitations of a temporary chemical effect. For some men topical testosterone replacement therapy is indicated based on what the bloodwork reveals. For many men a combination of both is the right approach. For some men the panel surfaces something that requires attention before anything else is addressed.
For men who complete the panel, the treatment plan is built around what it reveals. For men who start with Apex, bloodwork remains available and recommended at any point. In either case the plan follows from the individual's specific situation, not from a standard protocol applied to everyone who presents with similar symptoms.
If medication plays any role, it is one clinical tool among several, in a plan that was built around real information. Not the plan itself.
The Broader Point
There is nothing wrong with wanting a simple solution. The problem is that a simple solution applied to a complex clinical picture produces, at best, partial results, and at worst, a false sense that the problem has been addressed when it has only been temporarily managed.
Sexual dissatisfaction in men is almost always more clinically complex than a single prescription can account for. The men who get real answers are the ones who got a real clinical evaluation. The ones who found out what was actually driving what they were experiencing. The ones who built a treatment plan around that information rather than around the path of least resistance.
That is what is available. It just requires asking for it in a place that knows how to answer.
The Question Worth Sitting With
If you have been managing sexual dissatisfaction with medication for months or years, one question is worth asking honestly.
Do you know what's actually driving it?
Not what you assumed. Not what a brief appointment implied. Do you have a clinical picture of what is happening in your body, what the bloodwork shows, what the underlying factors are, and what a real treatment plan built around your specific physiology would look like?
Most men don't. Not because they haven't tried. Because the system they encountered was not designed to give them one.
That picture is available. It requires one blood draw and one honest clinical conversation. And it changes what is possible in ways that a prescription alone never could.
Springhouse Men's Wellness is a physician-founded practice led by Dr. Melissa Lee-Agawa. These articles are written by Taka Agawa, co-founder, with Dr. Lee-Agawa's clinical guidance throughout. Ambler, Pennsylvania. springhousemen.com